
Study suggests care gaps in people seeking help for self-harm
Understanding the care and support people receive after they have sought help for self-harm is vital. Appropriate and timely care can help prevent further self-harm and is key for suicide prevention. Most research to date has focussed on the role of mental health services, including outpatient care, psychological therapies, crisis home treatment teams and inpatient mental health services. However, general practitioners (GPs), voluntary, community and social enterprise (VCSE) services and social services can play a key role in providing self-harm aftercare. But do these services reach patients who most need them?
This study, led by Dr Sarah Steeg with contributions from researchers at the NIHR Greater Manchester Patient Safety Collaboration, set out to understand the types of services people were in contact with after self-harm, and which groups of people were experiencing possible gaps in care. To do this, we used information from a study on hospital attendances involving self-harm. We also held workshops with clinicians and people who had experience of self-harm services to co-develop measures of mental health and social needs of patients. We were able to examine the real-world care of over 26,000 patients, as well their potential care needs.
First, we found that six in ten (61%) patients were referred to their GP after attending hospital for self-harm. Nearly four in ten (37%) were referred to mental health services and 13% were referred to social or VCSE services. There was some overlap between the groups.
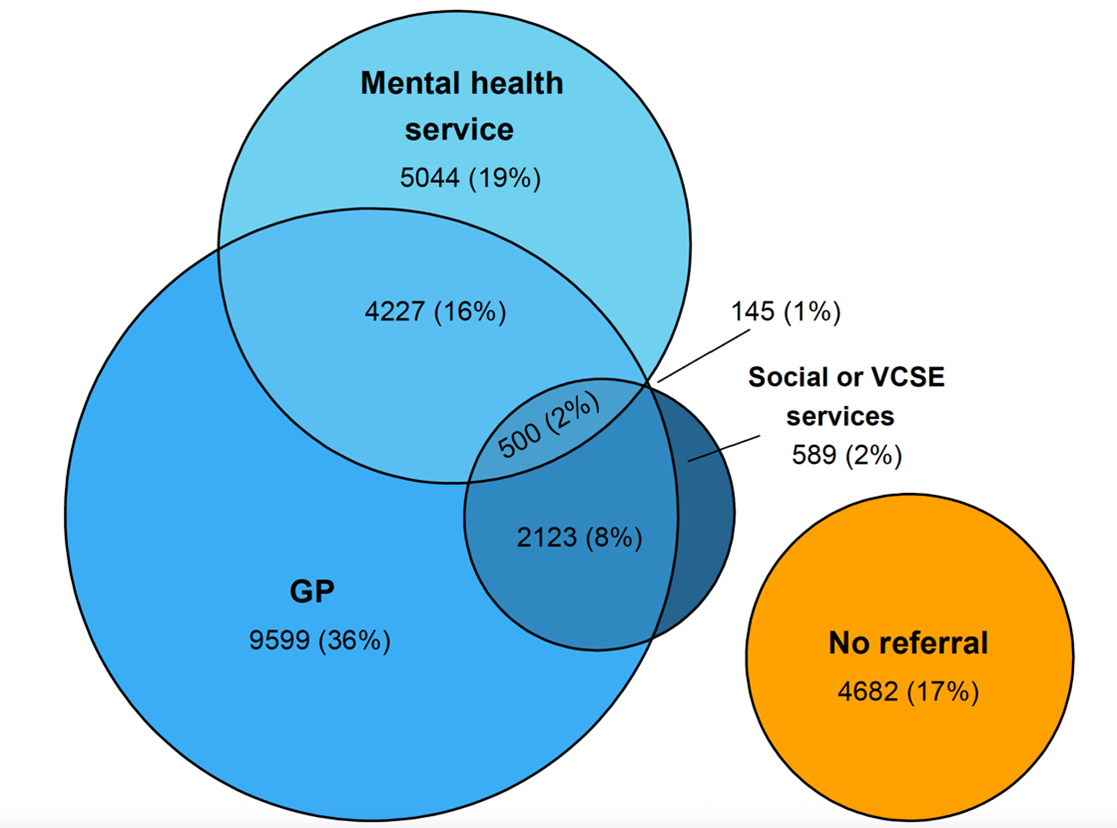
Venn diagram showing percentages of patients referred to their GP, to mental health services and to social or VCSE services following hospital presentation for self-harm.
GP, general practitioner; VCSE, voluntary, community and social enterprise.
Figure designed by Lana Bojanić (University of Manchester)
After examining information from clinical assessments, we found almost all (96%) had mental health needs but three in ten of these patients (30%) had no new or active referral to mental health services. And while just over half (53%) had significant social needs, eight in ten (80%) had no new referral to social and/or VCSE services, and almost a quarter (23%) also had no active or new referral to mental health services.
Then we looked at whether the level of unmet mental health or social needs varied between groups. This allowed us to estimate where care gaps (the percentage of patients who need care but do not receive it) were greatest. Mental health care gaps were largest for men, younger people, ethnic minority groups, those living in more deprived areas and people with alcohol or substance misuse disorders. Care gaps for patients with social needs were higher for men, people aged 45-64 and unemployed people. Importantly, many of these groups face increased risks of suicide.
Of course, people may get support from other places not captured in this study, for example from private or workplace services or family and friends. We also know that a referral to services does not necessarily mean that people’s mental health or social needs will be met. However, our findings suggest the provision of care may not be sufficient to meet people’s needs. Improving links between health, social and VCSE services may be a key strategy for closing the gaps and reducing inequalities in self-harm aftercare.
Funding: This work was funded by a Fellowship to Dr Sarah Steeg (award number: MHF009) as part of the Three NIHR Research Schools Mental Health Programme.






The University of Manchester
Oxford Rd
Manchester
M13 9PL
UK
Site hosted by The University of Manchester.
0 Comments